Key points
This framework is focused on the post-incident support response for staff following violence and abuse in the course of their work.
Preventing incidents is the priority, but it is not always possible; staff therefore need timely, practical and equitable support after an incident.
See the further reading section for post-incident guidance for both line managers and staff.
Introduction
Violence and abuse can occur in all healthcare settings, including community services and patients’ homes, and can affect any member of staff. Incidents can have a significant impact on health and wellbeing, including distress, trauma symptoms, burnout and reduced job satisfaction. Preventing incidents is the priority, but it is not always possible; staff therefore need timely, practical and equitable support after an incident.
This framework was commissioned by the national Social Partnership Forum (SPF). It is one of the recommendations of the SPF's report Ways to tackle and reduce violence against NHS staff.
It supports implementation of the NHS England violence prevention and reduction standard (VPRS), particularly standards 1.10 and 4.2, and should align with the NHS sexual safety charter and assurance framework. Multicomponent approaches (for example training, peer support and organisational commitment) are more effective than isolated interventions.
This guidance was developed by the Health, Safety and Wellbeing Group (HSWG) to establish a consistent approach to supporting NHS staff following incidents of violence and aggression by patients or members of the public whilst on duty. Both the SPF and NHS Staff Council endorse the guidance, and it should be used in collaboration with the VPRS to strengthen organisational responses and improve outcomes for staff.
What this framework covers
This framework covers the post incident support of staff following:
- physical violence
- verbal abuse
- online/digital abuse
- sexual assault
- sexual harassment.
This framework is focused on the post-incident support response for staff following violence and abuse in the course of their work. It is not intended to replace local safeguarding, HR, disciplinary, legal, or clinical incident management procedures.
Organisations should apply this framework alongside their existing policies and pathways, using professional judgement where incidents overlap.
Principles
The NHS should be a place where everyone has the right to work safely. Preventing violence and abuse is the priority, but we recognise incidents will still happen. When they do, staff should be supported quickly, consistently and with compassion.
- All incidents of violence, abuse, hate crimes and third‑party harassment against staff at work should be taken seriously and followed up with care and compassion.
- Violence and abuse can affect any staff group and any setting, including wards, community services, patients’ homes and remote/contact-centre roles.
- Some staff may be at higher risk of violence or targeted abuse, including women, black and minority ethnic staff, disabled staff and LGBTQ+ staff. Wider social trends (for example Islamophobia and antisemitism) may also increase risk for some staff groups. Support must be equitable and tailored to need.
- Staff recover better when they receive timely, appropriate support from their line manager and organisation.
- People respond differently. Previous trauma, cultural factors, personal circumstances, role experience and available support can affect how someone is impacted. Avoid assumptions and agree support with the individual.
- Organisations may need to invest in training, psychological support services and security resources to deliver an appropriate response.
- Leaders should set expectations, implement clear policies and procedures, and make sure staff receive timely support after incidents.
- Post‑incident support should be developed and improved in partnership with staff and trade unions.
- Where services are delivered by contracted staff (for example security where staff are likely to experience violence and aggression), the tender process should ask what post‑incident support will be provided and how their staff will access it (for example, via the contractor’s occupational health service or a service level agreement).
- Ensure staff are aware of potential financial support, including injury allowance, under their relevant NHS terms and conditions.
This framework describes practical ways to protect staff psychological safety and wellbeing after incidents of violence and abuse.
Be mindful that a ‘one-size fits all’ approach may not be effective and workplace support should be provided in a tailored and needs based approach for staff. Recognise that recovery may not be linear – workers may require different support at different times.
Definitions
Work related violence - Any incident in which a person is abused, threatened or assaulted in circumstances relating to their work. This can include verbal abuse or threats as well as physical attacks (Health and Safety Executive - HSE) and abuse via digital media towards staff. Actual threats or perceived threats of violence e.g. encountering weapons on a home visit, can also create fear and trauma in staff.
Behavioural related violence - These are violent actions and choices, and can be based on social or psychological factors, rather than underlying medical conditions. Behavioural cases often require security measures, behavioural agreements, and police liaison
Medically related violence – These arise from clinical or neurobiological conditions that impair cognition, perception, or emotional regulation rather than from deliberate intent. Sometimes called organic causes for violence and aggression, they may require clinical interventions, such as medication review, mental health support, or safeguarding protocols. They will require organisations to put in place controls around how we provide care whilst protecting staff safety.
Sexual assault - Sexual assault is when someone touches someone sexually without consent, with an object or body part.
Sexual harassment - Unwanted sexual comments, behaviour, or advances. Sexual harassment can happen to men, women and people of any sexual orientation. It can be carried out by anyone of the same sex, another sex or anyone of any sexual orientation.
Indecent exposure - Is when someone deliberately exposes their genitals to frighten or upset someone else.
Third party harassment – Under the Employment Rights Act* an employer must take all reasonable steps to prevent unwanted or offensive behaviour (related to protected characteristics of age, disability, gender reassignment, race, religion or belief, sex and sexual orientation), from a patient, relative or member of the public towards a member of staff.
(*Due to come into force in October 2026)
Hate crime - A hate crime is defined as 'any criminal offence which is perceived by the victim or any other person, to be motivated by hostility or prejudice based on a person's race or perceived race; religion or perceived religion; sexual orientation or perceived sexual orientation; disability or perceived disability and any crime motivated by hostility or prejudice against a person who is transgender or perceived to be transgender.'
A hate incident is any incident which the victim, or anyone else, thinks is based on someone’s prejudice towards them because of their race, religion, sexual orientation, disability or because they are transgender.
Planning
This section sets out what organisations must have in place before incidents occur to ensure staff receive timely and effective post‑incident support. These include policies, procedures, manager capability and governance.
- Ensure that violence prevention and reduction policies include clear protocols on staff support following a violent incident.
- Ensure there is a clear understanding by all staff (including agency, students on placement, volunteers and contracted staff) as to what constitutes a violent incident and how and when to report.
- Ensure the organisation raises awareness amongst all staff on the importance of incident reporting and what support they can expect after a violent incident (witness or victim).
- Ensure the organisation invests in training key staff (e.g. security staff, staff in high risk areas etc) to follow up violent incidents and support staff in providing evidence and completing incident reports.
- Ensure all line managers understand how to ensure staff receive post incident support, they must be aware of post incident support protocols and where to signpost staff to following an incident.
- Ensure the organisation has access to suitable psychological support services which are accessible to staff and appropriate to the level of need (e.g. size, risk – see Tehrani model for advice and guidance).
- Ensure the organisation builds links with local police services and is prepared to advocate for the member of staff by challenging a perceived or actual inappropriate response from the police service.
- Ensure the organisation recognises that some staff may be more reluctant to report incidents to police or to their organisation due to cultural issues or concerns about retaliation or the sensitivity of the assault e.g. sexual assault; and takes active steps to support staff with anonymised reporting in the case of sexual assault/misconduct (see sexual safety charter and assurance framework).
- Ensure the organisation has a route for confidential or anonymous reporting of incidents, such as Freedom to Speak Up or union representative, to give staff a way of speaking up if they feel unable to do so through normal routes.
- Ensure the organisation clearly sets out how staff can escalate concerns if they feel these have not been addressed by their employer — including via their union representative or Freedom to Speak Up Guardian.
- Ensure that where body worn cameras are used, there are appropriate governance arrangements in place.
Do
The stages of response:
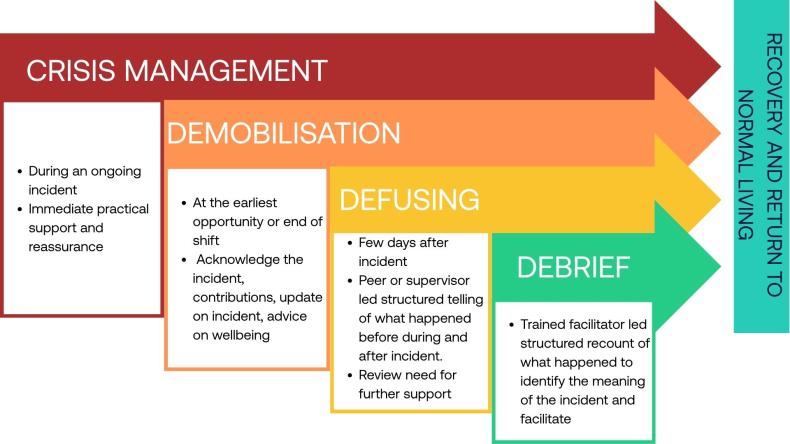
Not all the stages are necessary. Based on the incident and the individuals involved, at each stage consideration should be given to what further support is needed. For example, the information gathered during the demobilising/defusing stages may indicate where there is a need for debriefing led by a trained facilitator.
For many scenarios the earlier, and better, the provision of initial support will improve the time it takes for recovery and return to normal for individuals.
Crisis management/immediate response
Make the situation safe:
- Escalation both to security and clinical teams to ensure the violent behaviour has stopped, if required police or other services contacted for support.
First aid:
- Does anyone need support for physical injuries?
Basic psychological first aid:
- Does anyone need immediate emotional support?
- Is the staff member able to continue the shift?
- Can they continue their shift with reallocation of duties?
- If they can’t continue, do they need support to get safely home?
- Do they have a suitable support system at home?
- Ensure that a private (non-public facing) physical space is available for the staff to use in order to recover from the incident.
Reporting
Ensure the incident has been formally reported using organisational process. This can be the victim or a witness/manager or anonymously in the case of sexual harassment/assault.
If an incident is not reported in a timely manner it could lead to a delay in post incident support to staff.
Demobilisation stage
Immediately following the end of the incident or end of shift. It is a primary stress prevention conversation that takes place following a traumatic exposure. It involves a short conversation and is normally carried out by a supervisor or a suitably trained peer supporter.
- Safety and reassurance: Ensure the staff member (and anyone else impacted) feels physically safe and supported immediately after the incident. Assess ongoing risk and minimise the risk of any interactions of the perpetrator with the staff member who has been harmed.
- Clear communication: Thank people for their actions dealing with the incident. Updates on what is known, what actions are being taken (e.g., security, police involvement), and next steps.
- Advice on wellbeing: Acknowledge the traumatic event, remind people about common reactions after a traumatic incident and the potential impact of dealing with trauma. What the symptoms are, how to manage them and where to access further support.
Defusing stage
Ideally within three to ten days after incident. It helps assess who may need further help and support. Defusing is a small group process, less structured and aimed at the core group affected the most by the incident. Groups will meet with a line manager or peer supporter. Individual one-to-one sessions can be held if required.
- Structured telling of what happened before, during and after the incident: Understand the events and help people to understand.
- No-blame culture: Encourage open discussion without fear of reprisal; explore what was expected versus what happened.
- Offer further advice on wellbeing: Check in on the individuals and offer simple advice. If necessary, make a referral.
Debriefing
Ideally one to two weeks after the incident and is led by a trained facilitator to identify and understand the incident and facilitate recovery and return to normal living. It may identify individuals or groups who will require ongoing support.
After action review
An after action review (AAR) is a method of evaluation that is used when outcomes of an activity or event, have been particularly successful or unsuccessful. It aims to capture learning to promote improvements for the future. It is different from the psychological support and is around learning from the incident. The timing of this should be considered with trained facilitators who are supporting the teams to ensure it does not retraumatise staff. Following this, document lessons learned, actions required and share across teams to prevent recurrence.
Ongoing psychological support
- Access to occupational health and counselling: Offer trauma-informed care and referral pathways for those showing signs of distress.
- Peer support networks: Trained colleagues who can provide empathetic listening and guidance and sufficient space/facilities for staff to use for informal support.
- Monitoring for delayed reactions: Recognise that post-traumatic stress disorder (PTSD) or anxiety symptoms may emerge weeks later.
Organisational follow-up
- Review of risk assessment: This could include security reviews, local risk assessment reviews and individual patient care plans as appropriate.
- Policy updates: If required review against the VPRS standards as well as policies.
- Visible leadership commitment: Senior leaders should acknowledge the incident and reinforce that staff have a right to work safely.
- Support in reporting: The organisation recognises the fact that some staff may be more reluctant to report incidents to police or to their organisation due to cultural issues or concerns about retaliation or the sensitivity of the assault e.g. sexual assault; and takes active steps to support staff with anonymised reporting in the case of sexual assault/misconduct (see sexual safety charter and assurance framework).
- Unions: Share updates on organisational measures to support staff following a violent incident and ensure that union representatives are able to access anonymised data on violent incidents and follow up actions/outcomes of investigations.
Practical ongoing support
- Adjustments: Initial adjustments to duties may be necessary such as temporary redeployment. This should be done on a case-by-case basis taking into consideration any existing health needs.
- Legal and administrative help: Support with police statements, injury claims, and safeguarding referrals. Local policies should be adapted to allow time off for staff to attend court in relation to prosecutions without loss of earnings.
- Unions. Encourage staff to make early contact with their respective union reps for ongoing support.
- Police: If reported to police, ensure regular communication/updates on progress with case.
- Sickness absence: Absence related to a violent incident at work should not be subject to formal absence procedures/triggers. Sick pay provisions under section 14 of the NHS Terms and Conditions Handbook should be followed, with organisations paying due regard to the provisions within section 14.13.
- People teams or HR: Actively promote the financial support available to staff, including injury allowance, under their relevant NHS terms and conditions and external schemes such as the government’s industrial injuries disablement benefit. HR must provide clear guidance and support where injury allowance needs to be considered in line with relevant terms and conditions of employment.
- Line managers: Ensure staff are aware of potential financial support, including injury allowance provisions where absence may lead to loss of pay. If managers are unsure what support applies, they should signpost staff to HR for further advice.
- Line managers: Understand what the traumatic responses to violence are and how they may impact the mental health of staff and may not appear immediately after the event.
- Line managers: Regular welfare/wellbeing check ins with teams and staff who may have been affected by the incident including union reps who are supporting members who have been harmed or are on long term sickness absence.
- Line managers: Return‑to‑work support should ensure staff feel safe and informed. Managers must agree an individual return‑to‑work plan with the staff member, including any reasonable adjustments. Options may include a phased return in line with relevant terms and conditions of employment or temporary redeployment. Any additional learning needs required for a safe return should also be identified.
Reporting of incidents
Organisations must ensure that staff are actively encouraged to report all incidents of violence and aggression so that they can be given appropriate support and learning put in place to prevent recurrence. The organisation should ensure that:
- there is a consistent, systematic approach to all reported incidents
- this approach is documented in appropriate and relevant policies and processes
- the process highlights staff support as part of reporting of incidents of violence and aggression
- managers check-in on staff when they receive a report of an incident.
Support for reporting to police and being a witness in court
If staff are asked to give a statement to the police, or act as a witness in court it can make them relive the traumatic incident. Organisations should work with the police and The Crown Prosecution Service to minimise this.
When staff report a crime, the police will decide whether to carry out an investigation. If the police carry out an investigation this means that they’ll look for all the evidence so that they can understand what happened. The police will record the staff member's description of what happened – their witness statement. As part of their investigation, they will also take statements from anyone who saw what happened or who can provide information to help the investigation.
Statements should be collected by the police during work time, rather than after a shift or during the staff member's non-working hours (unless this is the preference of the staff member). Organisations should liaise with local police forces if this is not the case.
Trusts should ensure that there is a policy for how staff time is managed for attendance at court as a witness (either as the victim or a supporting witness called by the court). An example of best practice would be to provide staff with paid leave within special leave policies. This will encourage staff to report, as there will be no loss of income should they be required to act as witness.
An example from the Imperial College Healthcare NHS Trust special leave policy is below:
“If you’re required to attend court as a witness, you will be allowed to take paid leave, on the understanding that any payment that you get for loss of earnings from the court must be paid to us. You’ll need to provide evidence to us that you’ve been called as a witness.
There’s no entitlement to paid leave if you need to attend court as a defendant. You’ll need to request annual leave or unpaid leave if this is the case.”
Body worn cameras as primary evidence can avoid the requirement for staff to attend court in person.
Case study – safety cross to improve reporting
According to the NHS Staff Survey, one of the challenges in learning and supporting staff following violence and aggression is under-reporting of incidents. This could be due to several factors, such as time constraints or challenges accessing the reporting system.
Trusts have been trialling the use of a safety cross, which has been used in patient safety and other areas, to improve the capturing of incidents. It is a simple and quick method to record that an incident has occurred, so that a manager can report the full incident when there is time.
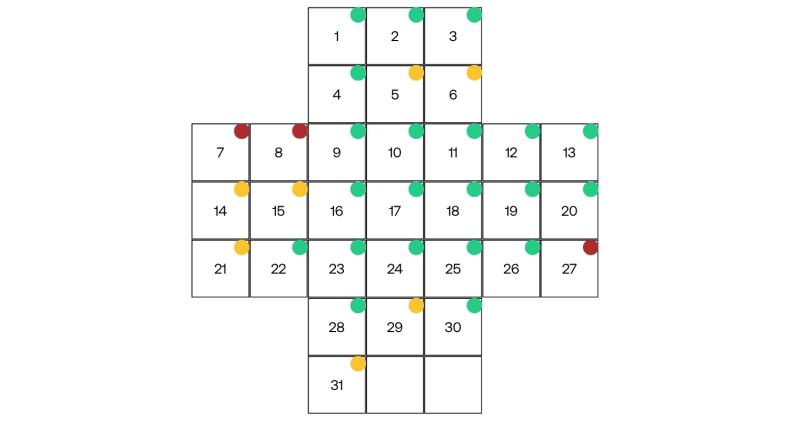
Each safety cross represents one calendar month, and each box represents a single day. At the staff handover the question is asked whether there were incidents of violence and aggression, whether they were reported on the incident reporting system, and checks if everyone is ok.
- Green dot equals no violence and aggression.
- Yellow dot equals verbal aggression.
- Red dot equals physical aggression.
The local manager then reviews this the next day, checks in on staff and ensures the details of the incident have been appropriately entered onto the local incident reporting system.
The safety cross is usually placed in an area that is visible to all staff so that people can:
- raise awareness of reporting violence and aggression
- look at how many days have gone by without an incident occurring
- spot patterns related to specific patients, workdays etc
- allow managers greater awareness of incidents that occurred when they are not on duty, so support can be provided
- ensure incidents have learning recorded to prevent recurrence.
Check
Staff receive timely responses to incident investigations, and where this may be prolonged by process requirement, this is recorded and communicated to staff, senior management and relevant stakeholders. When staff do not see outcomes, confidence in reporting drops which undermines staff psychological safety and culture.
- How is the timeliness and type of response to violent incidents evaluated and communicated to staff affected?
- Do staff impacted by violence, including witnesses, trust the organisation to support them and respond appropriately?
- How does the organisation support colleagues affected by violence?
- What support is available?
- What form does it take?
- Does this support reflect any statutory duty?
- What happens when investigations are delayed or prolonged?
- Is the best practice model followed for supporting staff, for example the Code of Practice for Victims of Crime in England and Wales?
- What stakeholder engagement processes are in place (such as with the police and Crown Prosecution Service) and how do they align with overall policy and communications with staff?
- What preventative multi-agency approaches could be adopted to work with perpetrators of violence as part of a public health driven, preventative approach?
Act
These standards support the implementation of the VPRS, specifically standards 1.10 and 4.2. Organisations should also link any post incident support activity with the requirements of the NHS Sexual Safety Charter and associated assurance framework.
Performance review - NHS organisations must undertake regular reviews of post‑incident support to ensure that senior management can direct and inform service improvements. Reports shall include both quantitative data and anonymised qualitative feedback to ensure the human impact is clearly understood.
Assurance and audit - Organisations must maintain assurance mechanisms to verify consistent delivery of post‑incident support. Regular audits shall assess if:
- welfare contact was made
- appropriate support was provided where indicated
- organisational learning actions were completed.
Audit findings shall be reported through established governance structures and used to drive continuous improvement rather than solely to demonstrate compliance.
Board oversight - Board scrutiny shall include active challenge on resource prioritisation and monitoring of agreed actions related to post‑incident support.
Annual management review - A senior management review must be undertaken annually (or as otherwise required) to assess the adequacy of post‑incident support:
- staff experience and themes affecting health and wellbeing
- outputs from staff surveys, focus groups
- evaluation of support processes and response times for counselling or employee assistance programmes
- analysis of anonymised staff feedback on support services
- timeliness of incident investigation and communication of outcomes
- outcomes of prosecutions or other legal proceedings.
Training and induction - Induction and mandatory training must outline the support available to staff following an incident. Managers and supervisors must be equipped with the skills required.
Resource allocation - Boards must be assured that psychological support, peer support programmes, and specialist services are sufficiently funded and accessible. Financial or operational pressures shall not be accepted as justification for inadequate post‑incident support.
Multi‑agency collaboration - Organisations should maintain active engagement with external partners, including police, safeguarding teams, local authorities, and mental health providers. Such collaboration supports shared learning, improves management of high‑risk individuals, and strengthens safety outcomes for staff and patients.
Models of support
Based on the size of the organisation you should implement and adopt one or more established models of post incident support (examples include):
Peer support programs - Formalised peer-to-peer support systems, which address emotional impact on healthcare workers after adverse events.
Reflective rounds - Regular multidisciplinary meetings focused on the emotional and social aspects of care, often used after distressing events.
Post Incident review panels - These panels have demonstrated an improvement in response time to incidents.
Personal impact statement - Provide opportunity for affected staff member/members to do a personal impact statement.
Case study - Peer support programs
At Imperial College Healthcare NHS Trust there is an in-house staff counselling service called CONTACT which offers counselling, stress management, conflict resolution and trauma support services.
They help support individuals and teams who have been involved in a traumatic incident at work. This might be a major incident, a one-off untoward incident, or a continuing stressful situation at work.
As part of this they have adapted peer support training, often used in military and police services to train managers and staff to provide immediate psychological support following a traumatic incident (‘demobilising’). Over 100 senior nurses and staff in the acute care teams were trained as peer supporters.
Peer supporter training covers:
- recognising and understanding the nature and causes of traumatic stress
- identifying the main symptoms of trauma
- developing and learning skills to demobilise and defuse situations
- knowing when there is a need for a referral to further/specialist support - how and where
- recognising and looking after own needs.
This formalised peer-to-peer support system addresses emotional impact on healthcare workers after adverse events and allows someone to be on the spot at all shift times to support with defusing and debriefing.
All these interventions aim to minimise the likelihood of developing post-traumatic stress disorder (PTSD) and enable staff to get the support they need.
Case study - Reflective rounds
Regular multidisciplinary meetings focus on the emotional and social aspects of care, and are often used after distressing events.
Reflective rounds are a powerful opportunity for all staff – across divisions, specialisms and hospitals – to come together to share stories and reflect on different themes and topics.
A panel comprised of a small group of staff, share their experiences at the start of the session. Following this, trained facilitators lead an open reflective discussion, ensuring the space retains psychological safety and confidentiality, and that the session does not become about problem solving.
They are an opportunity for staff to interact and connect with colleagues – at the heart of each session is a focus on providing truly compassionate care and looking at how our staff, as humans, are impacted by their work and interactions with patients.
Reflective rounds fall into two main categories:
- open trust rounds which are online facilitated meetings
- smaller departmental rounds which are in-person facilitated meetings.
After listening to a panel’s brief presentation on an identified case, theme or topic, staff in the audience are invited to share their own perspectives and experiences, and the things that have resonated with them or any related issues.
However, there is no pressure for staff to share their experiences directly. There is real value in coming along to listen and being present in a safe space where people can be truly vulnerable.
This format allows for a free exchange of ideas, feelings and reactions, reinforcing the common humanity of caregivers, patients and families and paving the way for meaningful conversations.
Case study - Post incident review panels
The use of weekly incident review panels in hotspot areas like A&E which are made up of:
- clinical teams
- security
- mental health
- substance abuse
- homelessness
- learning disability team
- safeguarding
In addition, some trusts have police, probation services etc as part of this.
These panels have demonstrated an improvement in response time to incidents. The panel looks at what happened, staff support, restraint used, de-escalation opportunities, further sanctions, electronic patient record (EPR) alerts, care plan, additional support the patient may require, external service referral etc. This then means a response to the reporter is sped up with actions aimed at preventing recurrence.
For lower risk areas or small organisations, it may not be appropriate to have a weekly meeting. However, having a core group multidisciplinary team (MDT) who can review more complex cases on an ad hoc basis will support timely investigations and feedback to staff.
Violence and aggression review panel
| Frequency | Weekly |
| Venue | Online (MS Teams) |
| Composition | Site specific multidisciplinary team, roles covering:
|
Pre-meeting:
- Incidents will be reported via incident reporting platform by staff in the A&E department.
- A member of the MDT team will ensure incident data is collected in an excel database – shared using SharePoint among all in attendance.
- The excel database includes a list of open and closed incidents, as well as closed and open actions originating from these incidents.
Meeting:
- The meeting starts with an update on open actions (listed on excel database).
- The meeting will then review all incidents reported during the last week following a situation, background, assessment and recommendation (SBAR) approach.
| Situation | Incident is reviewed directly from the incident record – including actions implemented post-incident and, where relevant, an overall picture of A&E at the time (for example, presence of other patients displaying challenging behaviours). |
| Background | Incident is reviewed, using information listed on electronic patient record notes and incident report. Consideration is given to:
|
| Assessment | Establish key findings and learning from the incident, focusing on measures targeting:
|
| Recommendation | MDT team defines actions required (e.g. review of SOPs, training needs, workflows, A&E/security, etc.) Teams will also:
|
Other organisations who can provide support to staff
Further reading
- NHS staff standards guidance
- Social Partnership Forum (SPF) - Ways to tackle and reduce violence against NHS staff
- Royal College of Nursing (RCN) - RCN's position on work related violence in health and social care.
- Cambridge University Press - Analysis and evaluation of peer group support for doctors in postgraduate training following workplace violence and aggression.
- Liverpool John Moores University - Work-based violence, harassment and abuse towards NHS staff in England.
- Strategies to Reduce the Impact of Trauma in Psychiatric Nurses: An Integrative Review of the Literature.
Guidance for managers and staff
To support this framework, two additional checklists have been developed:



